Melanoma is the most serious common form of skin cancer, and its incidence in the UK has been rising steadily for several decades. It is now one of the most frequently diagnosed cancers in young adults, and the British Isles consistently record some of the highest rates in Europe. The reassuring news is that when melanoma is found early, outcomes are excellent; prevention and early detection remain the single most effective tools we have.
This article is a plain-language overview of what melanoma is, why rates are climbing, the risk factors that matter most, and the practical prevention strategies that genuinely make a difference. It is written for patients and their families, not for clinicians, and it is deliberately focused on what you can actually do.
What is melanoma?
Melanoma is a cancer that arises from the melanocytes, the pigment-producing cells of the skin. It can develop in an existing mole, but more commonly it appears as a new mark on apparently normal skin. Because melanocytes also live in the eye, the mouth and the soles of the feet, melanoma can occasionally appear in areas that never see the sun. Most melanomas, however, develop in skin that has been repeatedly exposed to ultraviolet radiation.
Why UK rates are rising
There is no single reason for the increase, but several trends overlap. Package holidays and cheap flights have made intense sun exposure routine for a population whose skin often evolved for cloudier weather. Sunbed use, though declining, still contributes significantly. Greater public awareness and better detection also capture cases that might once have gone undiagnosed. Importantly, the rise is not inevitable. Countries that have invested in serious public health campaigns have begun to flatten their curves.
Key risk factors
Risk factors for melanoma cluster around how much ultraviolet radiation the skin has absorbed, how vulnerable that skin is to damage, and individual biology. Knowing where you sit across these factors helps you decide how aggressively to protect yourself and how often you should be having your skin checked.
Ultraviolet exposure
- Intense intermittent sun exposure: holiday sunburns, particularly in childhood, are more strongly linked to melanoma than steady year-round exposure.
- Sunbeds: the use of tanning beds before the age of thirty-five substantially increases the lifetime risk of melanoma. There is no safe level of sunbed use.
- Outdoor occupations and hobbies: prolonged exposure over many years is a significant factor, especially without consistent sun protection.
Skin type and personal features
- Fair skin, light eyes and red or blonde hair: skin that freckles or burns easily is more vulnerable because it contains less protective melanin.
- A high total number of moles: patients with more than fifty moles, or with several atypical moles, carry an increased risk.
- Previous skin cancer: a history of melanoma or non-melanoma skin cancer raises the risk of a further cancer developing.
Family history and biology
- A first-degree relative with melanoma: a parent, sibling or child with melanoma roughly doubles the risk and sometimes reflects an inherited genetic tendency.
- Immunosuppression: patients who have had organ transplants or who take long-term immune-modulating medication have a higher risk of skin cancers, including melanoma.
- Older age: although melanoma can affect young adults, incidence rises steadily with age as cumulative damage adds up.
Prevention that actually works
The evidence for prevention is strongest for measures that reduce ultraviolet exposure and for measures that help find cancer early while it is still completely curable. The two go hand in hand.
Sunscreen, used properly
A broad-spectrum sunscreen protecting against both UVA and UVB, with an SPF of at least thirty, is a cornerstone of prevention. The single biggest mistake I see is not the choice of product but the quantity applied. Most people apply around a quarter of the amount used in laboratory testing, which reduces the effective SPF dramatically. Re-application every two hours, and after swimming or heavy sweating, matters as much as the initial application.
Clothing, shade and timing
Textiles block ultraviolet radiation far more reliably than sunscreen. A hat with a proper brim, sunglasses with UV protection, and a light long-sleeved top are simple and effective. Avoiding direct sun between about eleven in the morning and three in the afternoon, particularly in spring and summer and at altitude, meaningfully lowers exposure.
Say no to sunbeds
The evidence against sunbeds is now strong and consistent. They are classified by the World Health Organization as carcinogenic to humans. There is no cosmetic benefit that justifies the risk they pose.
"Early detection remains the most powerful tool we have. A melanoma caught in its first millimetre of growth is almost always curable with a simple operation."
Checking your own skin: the ABCDE rule
Monthly self-examination takes only a few minutes and can make a real difference. The ABCDE rule is a useful framework for spotting changes that deserve review.
- A is for Asymmetry: one half of the mole does not match the other.
- B is for Border: edges that are irregular, ragged or blurred.
- C is for Colour: a mixture of shades or a recent change in colour.
- D is for Diameter: lesions larger than six millimetres, roughly the size of a pencil rubber.
- E is for Evolving: any mole that is changing in size, shape, colour or symptoms such as itching or bleeding.
A useful additional concept is the ugly duckling sign. Most of our moles tend to look like each other. A lesion that stands out as different from its neighbours is worth showing to a doctor even if it does not tick every ABCDE box.
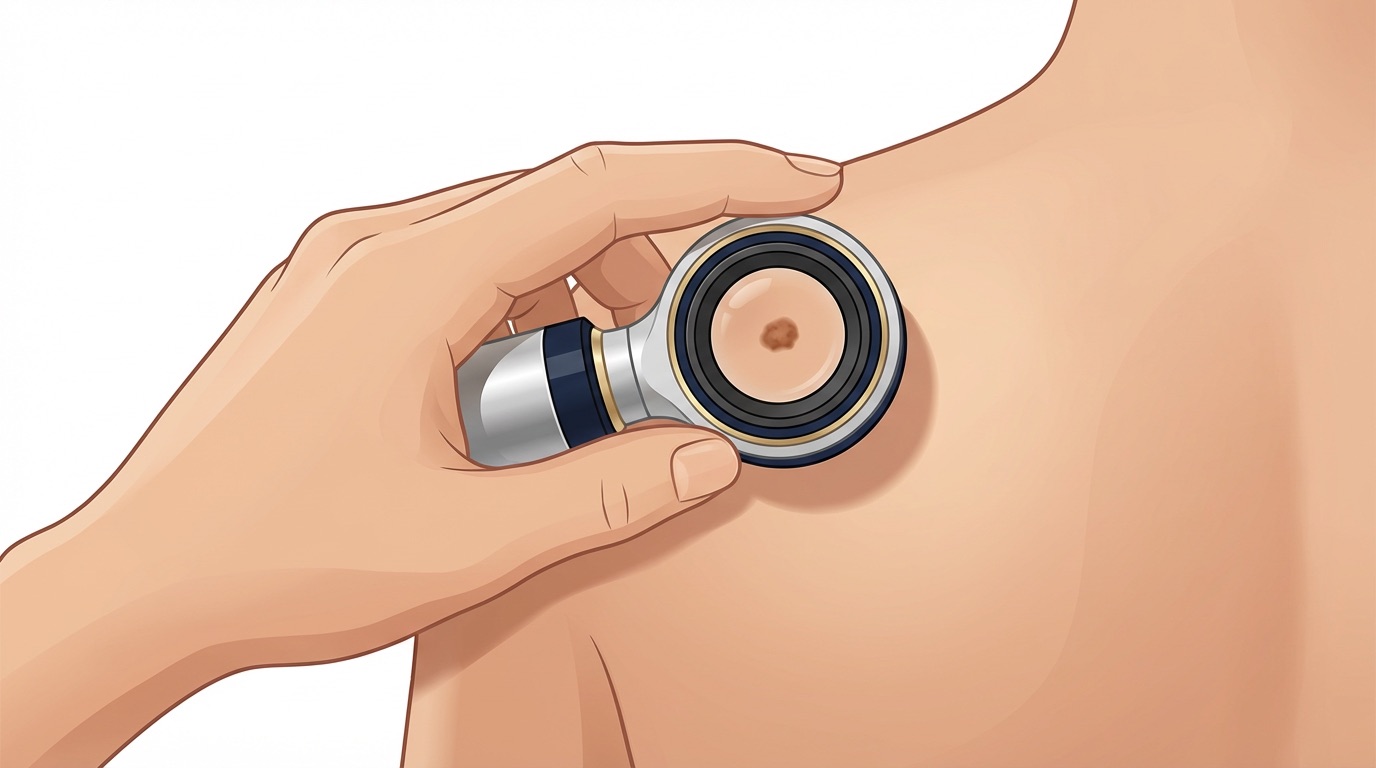
Professional checks and mole mapping
For patients with many moles, a personal or family history of melanoma, or atypical-looking lesions, professional skin examination offers an extra layer of reassurance. Dermoscopy, in which a specialised magnifying device is used to look at a mole in detail, allows features invisible to the naked eye to be assessed. In selected patients, total-body photography and digital mole mapping can track subtle changes over time and reduce the need for unnecessary biopsies.
When to seek specialist review
Any new, changing or symptomatic mole deserves attention. You should seek a review if a lesion is growing, changing colour, bleeding, itching, crusting, or simply looks different from the rest of your moles. If your GP (General Practitioner) is concerned or uncertain, they will refer you for specialist assessment. Private specialist review is also available and can often be arranged quickly, which is particularly valuable when a lesion is causing anxiety.
A hopeful conclusion
It is easy to feel daunted by melanoma statistics, but the most important number to remember is this: when melanoma is diagnosed at its earliest stage, the long-term survival rate is very high. Prevention and early detection truly save lives. Sensible sun habits, an honest eye for change and prompt professional review when something looks different are the pillars of protection. If you have concerns about a specific mole or your overall skin cancer risk, please book a consultation for a thorough skin assessment.