Inverted Nipple Correction
Inverted nipple correction is a short surgical procedure that releases tethered ducts and fibrous bands beneath the nipple to allow it to sit outwards in a natural projected position.
Overview
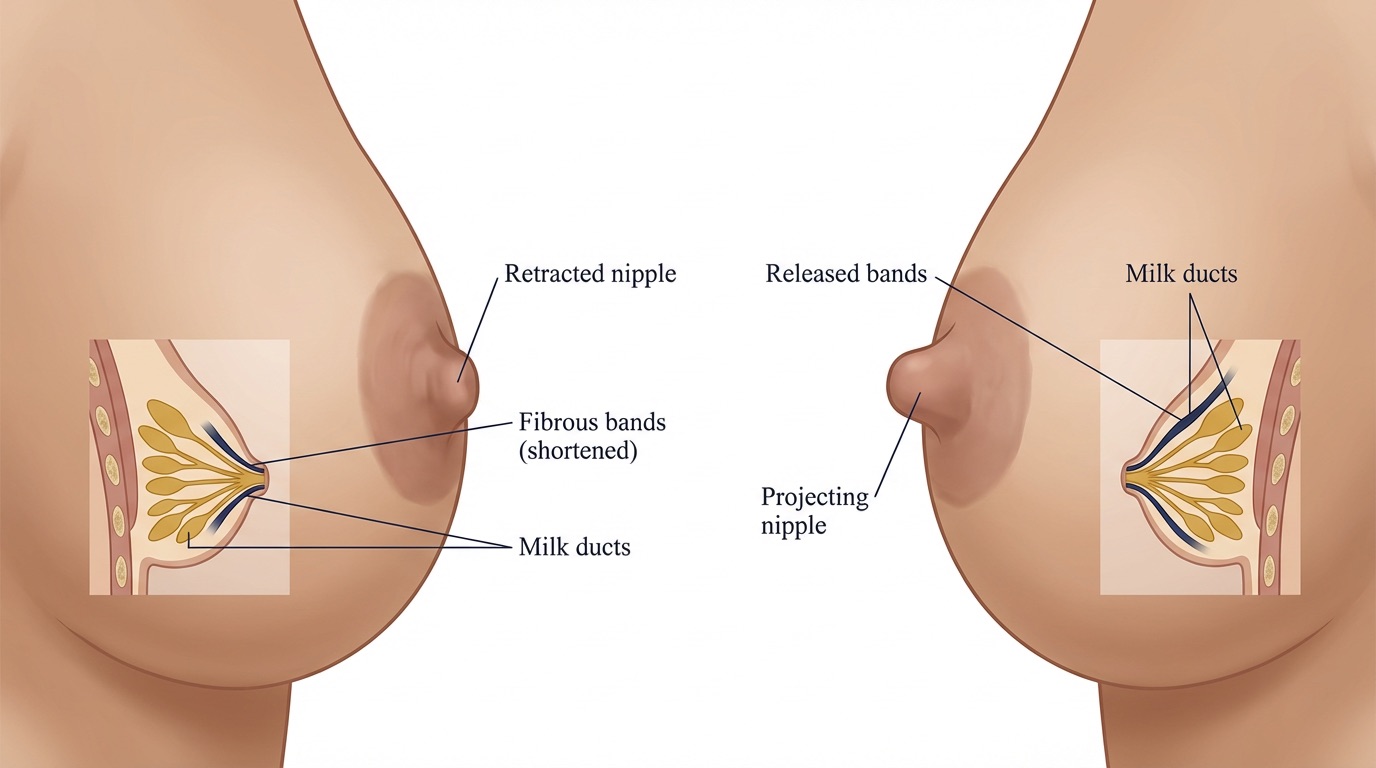
Inverted nipples occur when the nipple is retracted inwards rather than projecting outwards from the areola. This can affect one or both sides, and may be present from puberty or develop later in life. Most cases are caused by shortened milk ducts and tight fibrous bands pulling the nipple inwards; less commonly, inversion can be a sign of an underlying breast condition, which is why a careful clinical assessment is always performed first.
Inverted nipple correction is a straightforward day-case procedure designed to release these tethered ducts and fibrous bands, allowing the nipple to sit in a natural, outward-projecting position. It can be performed on its own or in combination with other breast procedures. Mr Singh will discuss the degree of inversion (often classified as grade 1, 2 or 3) and the most appropriate technique during your consultation.
Benefits
- Improved nipple projection: The nipple is released to sit in a natural, outward position.
- Enhanced breast appearance: A more symmetrical, aesthetically pleasing look of the nipple-areolar complex.
- Relief from irritation: Reduction in hygiene issues, skin irritation or recurrent discharge associated with persistently inverted nipples.
- Short procedure with quick recovery: Typically performed as a day case under either local or general anaesthetic, allowing a rapid return to normal activities.
- Minimal, well-hidden scarring: Incisions are small and placed at the base of the nipple, making them inconspicuous once healed.
- Boosted confidence: Many patients describe significant improvement in self-confidence and comfort with their appearance.
Surgical Techniques
The procedure is usually performed under a local anaesthetic or under a general anaesthetic as a day case, taking around 30–60 minutes. The precise technique depends on the degree of inversion and whether you wish to preserve the ability to breastfeed in the future.
- Small Base Incision: A tiny incision is made at the base of the nipple, hidden in the natural pigmented border of the areola.
- Release of Fibrous Bands: The tight fibrous bands responsible for pulling the nipple inwards are carefully divided to allow the nipple to project outwards.
- Duct-Preserving Technique: Where possible, and especially in patients who may wish to breastfeed in the future, the milk ducts are preserved during release.
- Duct Division Technique: In more severe or recurrent cases (grade 3), division of the shortened milk ducts may be necessary to achieve a lasting correction; this will affect the ability to breastfeed from that nipple.
- Internal Sutures: Fine dissolvable sutures are placed beneath the nipple to support the new projected position and reduce the risk of recurrence.
- Closure and Dressings: The skin is closed with fine dissolvable sutures and a small protective dressing is applied around the nipple.
Risks & Considerations
General Risks
- Infection: Risk of wound infection which can delay healing and require antibiotics.
- Bleeding or bruising: Minor bleeding or bruising around the nipple is common and usually settles quickly; significant bleeding is rare.
- Scarring: Small scars at the base of the nipple which are typically well concealed and fade over time.
- Local anaesthetic reactions: Rare allergic or sensitivity reactions to local anaesthetic agents.
Specific Risks to Inverted Nipple Correction
- Recurrence of inversion: The nipple may partially or completely re-invert over time, particularly with grade 3 inversion; further surgery may occasionally be required.
- Changes in nipple sensation: Temporary or permanent changes in sensation, including numbness or hypersensitivity.
- Inability to breastfeed: When ducts are divided to achieve correction, breastfeeding from that side is unlikely to be possible.
- Asymmetry: Slight differences in projection, shape or size between the two nipples.
- Nipple ischaemia or loss: Very rare loss of blood supply to the nipple, which can result in partial or total nipple loss.
- Scar thickening: Occasional development of firm or raised scars in the healing area.
Recovery
Garments
- Protective Dressing: A small dome or shield dressing is often used over the nipple to protect it from pressure and maintain projection during the early healing phase.
- Soft Bra: A soft, non-underwired bra can be worn for comfort.
Wound Care
- Dressings: Keep dressings clean and dry and follow specific instructions about when they can be changed.
- Cleaning: Once permitted, gentle daily cleaning of the area with mild soap and water helps to reduce the risk of infection.
- Activity: Most patients return to light daily activities within 24–48 hours and to desk-based work within a few days.
Scar Advice
- Scar Care Products: Once the wounds are fully healed, silicone gels or moisturisers can be applied to help minimise scarring.
- Sun Protection: Protect the area from sun exposure while the scars are maturing.
- Massage: Gentle scar massage, once healed, can help to soften and flatten any residual scarring.
Follow-Up
- Initial Post-Op Visit: Typically scheduled around 1–2 weeks following surgery to check on wound healing and remove any protective dressings. Sutures are usually dissolving.
- Subsequent Visits: Usually seen again around 6 weeks following surgery for an early check and at approximately 3 months for a longer-term review of projection and symmetry.
- Long-Term Care: Mr Singh remains available for any concerns, including any signs of recurrence or further follow-up as required.
Procedure Summary
Ready to Discuss Inverted Nipple Correction?
If you are considering inverted nipple correction, please feel free to contact us to answer any questions you may have or to schedule a consultation and learn more about how this procedure may benefit you.
Book a Consultation